Does pay for performance work to improve immunization coverage?
Authors: Ivdity Chikovani
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services. P4P can be employed as an approach to incentivize health care providers to improve service delivery outcomes. As policymakers in Georgia consider P4P as an approach to address primary health care (PHC) challenges, they commissioned a review of the existing evidence in the literature to inform policy discussions. The findings of that review are summarized below.
In high-income countries, P4P has been applied to achieve better quality care and greater cost savings, while in low- and middle-income countries, P4P has primarily been used to increase utilization of care. P4P has been extensively researched worldwide and has been a subject of debates between researchers and policymakers. In general, studies from the 1990s through 2000 tend to show more positive results on the effectiveness of P4P, while later studies show less favorable outcomes. This is attributed to more rigorous methodologies used in study design and analysis. [1], [2]

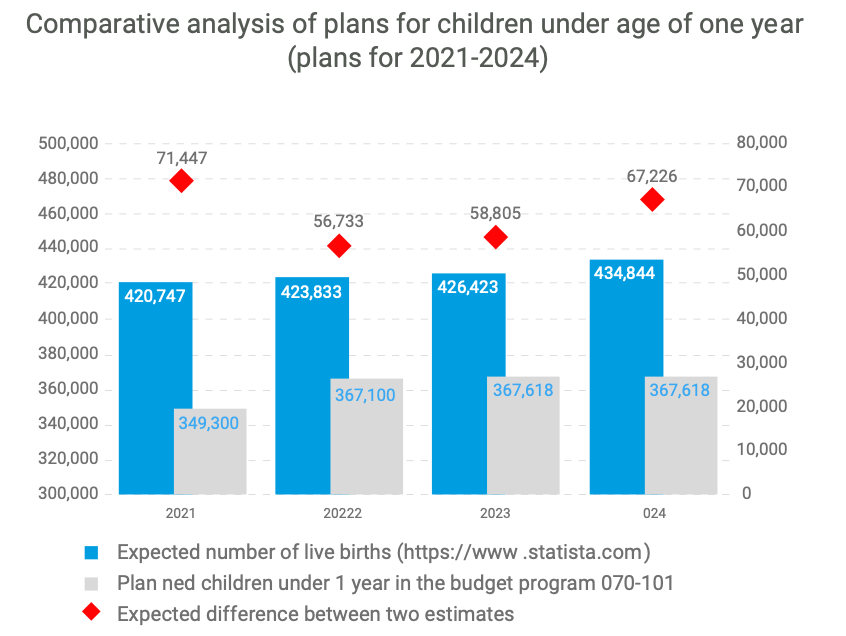
The variation in results is found not only across countries, but even within programs, highlighting the importance of the specific context. A study in Nigeriashowed that the P4P scheme implemented in three states resulted in an increase of the average coverage for completely vaccinated children from 1.4% to 49.2% during the two-year period with variation between the states (between about 40% to 80%),[5]Although all three states had similar starting coverage points and a similar scheme design, differences in management processes, staffing, and involvement from community leaders resulted in differences in performance improvement. [6] Additionally a study in the United States found a significant increase in coverage for eight out of ten vaccines and no change for two vaccines with starting coverage rate around 80%.[7] On the other hand, a study in Rwandademonstrated that P4P was no more effective than the existing payment method to increase full immunization coverage, and a Canadian study revealed that the P4P did not produce significant changes in immunization coverage. [8], [9] In Canada, a small incentive size in relation to base income, and concurrent changes to base payment methods may have diluted the income effects, resulting in poor response to the incentives. [9]
There are still many uncertainties with regards to P4P despite extensive research – like what is the optimal bonus size to create enough motivation while avoiding diminishing of intrinsic motivation? What is the optimal number of indicators to measure performance and avoid overburden of reporting? Is the P4P model cost-effective?[3] P4P programs can also generate unintended consequences, such as deterring health professionals from performing other activities, fabrication of the results to receive higher incentives, administrative burden, and crowding out of intrinsic motivation. Thoughtful design is needed to avoid these outcomes and a good monitoring system should be in place to capture manipulation of the results. Accountability and performance feedback to managers and providers is critical to facilitate performance improvement.
Despite mixed evidence, there is sufficient evidence demonstrating that P4P can improve immunization program performance in some settings. Careful consideration of important factors suggested by the evidence will help program planners ensure their desired outcomes are achieved.
This blog was published with permission from LNCT. The original version found here: https://lnct.global
Latest News
Integrated Bio-behavioral surveillance and population size estimation survey among Female Sex Workers in Tbilisi and Batumi, Georgia, in 2024
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.









CIF and the Results for Development / Accelerator combined their expertise to co-author an insightful blog, shedding light on Georgia’s commendable efforts to overcome limited data challenges and develop evidence-based policies for financing rehabilitation services
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.

Culminating event – Building Institutional Capacity for Health Policy and Systems Research and Delivery science (BIRD) in six WHO Regions
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.





New case study: Sustaining effective coverage with Opioid Substitution Therapy (OST) in Georgia in the context of transition from external assistance
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.








Data Analysis and Synthesis Workshop – analyzing the implications of the structure of Georgia’s private healthcare market for quality and accessibility
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.





Article: How do participatory methods shape policy? Applying a realist approach to the formulation of a new tuberculosis policy in Georgia
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.





Effects of Pay for Performance on utilization and quality of care among Primary Health Care providers in Middle and High-Income countries
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.


The first phase of the joint fellowship program of the Curatio International Foundation and the Knowledge to Policy Center (K2P) at the American University of Beirut has been successfully implemented
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.
Concentration and fragmentation: analyzing the implications of the structure of Georgia’s private healthcare market for quality and accessibility (ConFrag)
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.






LNCT Webinar: Implementing a High Performing Immunization Program within the Context of National Health Insurance: What can we Learn from Thailand?
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.














Memorandum of Cooperation between the Health and Social Issues Committee of the Parliament of Georgia and Curatio International Foundation
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.







Technical Assistance for evaluation of transition readiness and preparation of Transition and Sustainability Plan for Global Fund-supported programs in Tajikistan
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.


Article: Barriers to mental health care utilization among internally displaced persons in the republic of Georgia: a rapid appraisal study
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.



Article: Barriers to delivering mental health services in Georgia with an economic and financial focus: informing policy and acting on evidence
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.

Conference paper: The Study of Barriers and Facilitators to Adherence to Treatment among Drug Resistant Tuberculosis Patients in Georgia to Inform Policy Decision
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.
Conference paper about realist evaluation: Informing policy, assessing its effects and understanding how it works for improved Tuberculosis management in Georgia
Pay for Performance (P4P) is a financing mechanism that has flourished in recent years as countries look for innovative ways to improve coverage of health services.